Psoriatic Arthritis Treatment in Bangalore: What You Must Know
Introduction to psoriasis and psoriatic arthritis
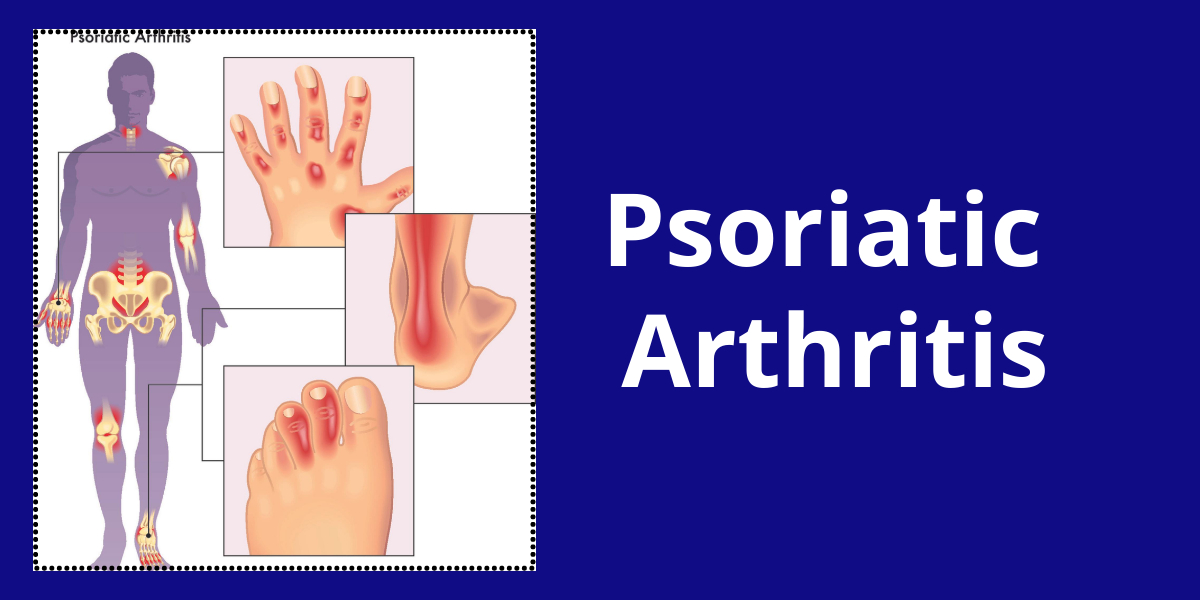
Psoriasis is an autoimmune skin disease. It is a skin disease. To say it is an autoimmune reaction, showing its symptoms on the skin. But it also predominantly affects other parts of the body with an increase in severity. One such consequence is Psoriasis-Arthritis.
It is commonly found in patients living with psoriasis. It is a kind of oligoarthritis with lesser and characteristic features of its own. Arthritis is an inflammation of joints, stiffened and swollen joints. People with psoriasis catch up with arthritis which is called psoriatic arthritis.
Psoriatic arthritis is as chronic as psoriasis but has manageable treatments and medications. All those efforts can reduce the impacts and symptoms but cannot cure the disease completely. One in five patients living with psoriasis has psoriasis arthritis.
The prevalence of psoriasis arthritis ranges from 0.16 to 0.25 percent. About 20 to 30 percent of the patients with psoriasis are affected by psoriasis arthritis. However, it may vary in different populations.
Onset and symptoms of psoriatic arthritis
- Psoriatic Arthritis starts within no time along with psoriasis. In a few cases, say in about 15 to 20 percent of patients, arthritis can develop even before psoriasis signs are noticeable on the skin and other parts of the body. Psoriasis appears first in 60 to 80 percent of psoriasis arthritis cases. Occasionally both of them appear together.
- These musculoskeletal symptoms are mostly insidious in many even after the onset. Some others may experience only stiffness and pain of the joints. Although the symptoms seem easy, about one-third of the patients have reported acute onset of the disease.
- Rheumatoid arthritis and psoriatic arthritis are both synonymous in signs and symptoms. Both conditions develop sore and painful joints that are swollen. Both the joints or only one of them can be affected in this situation.
Major Signs and changes in the body:
- Fingers of hands and toes are swollen, painful, and look like sausages as in dactylitis in 35 percent of patients.
- Skin lesions, nodules, erythematous skin and plaques, guttate lesions, nail psoriasis and nail traumas, inverse psoriasis, lakes of pus, and microtraumas happen in psoriatic arthritis alone.
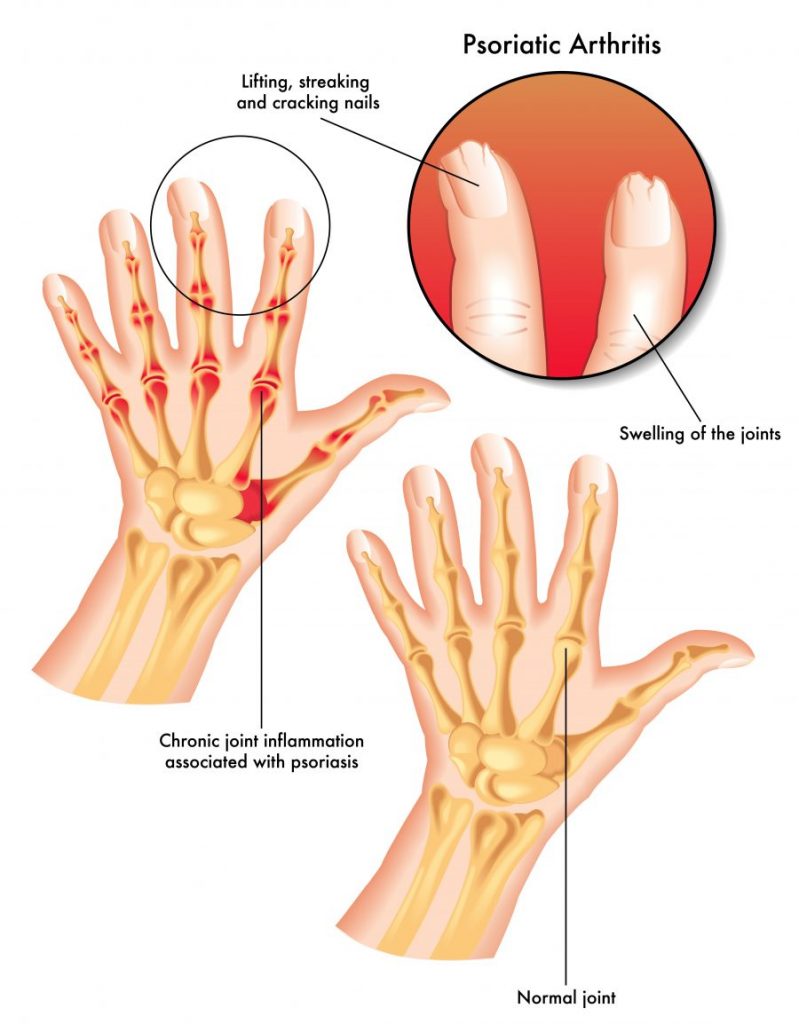
- In some cases, the fingers and nails might develop deformities. The time where the worsening of disease signs in the fingers starts is also the beginning of psoriatic arthritis.
- Enthesitis of the ligaments, tendons, insertions into bone, Achilles he dons, plantar fascia, and cancellous bone are one sign of psoriatic arthritis.
- Cracking of the edges of the nail, pitting of the nails uniformly, ridging on the nails transversely, the appearance of tiny blood dots under the nails, half moon nails, hyperkeratosis, beau lines, etc are the nail changes in the psoriatic arthritis
- Fatigue happens because the body gets drained of energy with the painful joints, inflammation, and also the tiring medications that are taken to get down psoriatic arthritis.
- Exercise, eating, and sleeping well make a person feel better.
- Rib and chest pains, as said because the ligaments of the rib cage and cartilage of the chest bone also get affected in psoriatic arthritis.
- In the rarest instances, the blood vessels of the heart also called aortas can get affected.
- Nails, get separated from the nail bed, get deformed to greater extents, pits, and ridges are formed on the nails.
- Discoloration of the nails, and onycholysis cause yellowish and green nails. Dents in the nails can be noticed.
- Subcutaneous nodules are rare but also present in psoriatic arthritis.
- Conjunctiva of the eyes may get involved by 20 percent, ocular involvement by 30 percent, and 43 percent of the sacroiliitis may be involved in psoriatic arthritis
- Psoriasis affects almost one percent of the total population. In almost five percent of the psoriatic Arthritis cases, the joints in the feet and hands get deformed.
What is psoriatic arthritis?
Psoriasis itself is an autoimmune disorder, which means parts of the body are attacked by unwanted immunity responses created by our immune system. Beyond this, the joints and bones also get utterly damaged and in some cases get disabled to a complete extent. This causes inflammation in the joints and bones making them painful, sore, stiffened with swollen appearance. The tissues and ligaments associated along with those bones and joints at their articulations will be damaged in extreme cases. This can be of two types based on the severity and number of joints affected. Psoriatic arthritis, in general, can affect only one joint or both joints in a person.
There are various patterns in which psoriatic arthritis appears and affects people. They are listed and defined as follows
Asymmetric psoriatic arthritis
- It is a type of psoriatic arthritis, in which both the joints of the same side are affected. It can be told as both left joints or single joints. It is milder in general with almost 35 percent of psoriatic arthritis cases.
- To be precise it is asymmetrical oligoarticular arthritis. It was considered the most prevalent type of psoriasis arthritis for a long time.
- The characteristic sausage like the appearance of the fingers and toes as in dactylitis happens in these patients but asymmetrically. The inflammation starts at the digits of the fingers of both hands and feet, alongside the tendons.
- The knee joint is also seen being affected. The flexions get affected too. Lesser than five joints are affected in this type of psoriasis arthritis.
Symmetrical psoriatic arthritis
- This is a condition in which the same joints are symmetrically attacked from both sides. This looks like rheumatoid arthritis. Bone deformity and impact on the bones are both low and mild. Almost half the psoriatic arthritis cases are of this kind.
- This is a severe type of arthritis in which more than four joints are involved and is also the most common one too. Unlike asymmetrical oligo articular psoriasis, this is symmetrical.
- Also, it is the one that can differentiate psoriatic arthritis from rheumatoid arthritis.
- The inflammation of distal toe tip joints also called distal interphalangeal joints, the symmetrical pattern, the absence of deep lesions unlike rheumatoid arthritis, and also testing negative for the rheumatoid factor.
- Also, symmetrical polyarthritis is milder than rheumatoid arthritis.
- Psoriatic arthritis brings along with it spondylitis, dactylitis, and enthesitis, though they seem individual. They are given the names based on the target attacking sites of psoriatic arthritis in our body.
Distal interphalangeal arthritis
- The pain in the distal joints of fingers, the inflammation, and also the obvious inflammation of the nail bed, swelling, stiffness, and tuft of the digital are the characteristics of this type that make it difficult to differentiate it from arthropathy.
- It affects the joints nearer to the nails, which means the distal end joints
- It is seen more often in men.
- It is a rare type of psoriatic arthritis with fewer percentage of people being 10% of psoriatic arthritis cases.
Dactylitis
- This is a condition of fingers and toes, in which they become sausage-like swollen, deformed. The ligaments and tendons around them get inflamed. It is more frequent in the feet and also in the second digit of the hands.
- There can be lesions, high chances of injuries, and micro-traumas in this type of psoriasis arthritis. The flexor tendons thicken constraining movements. But in severe conditions of dactylitis, the fingers can also be deformed which is a serious and strong symptom of psoriatic arthritis.
- Even though this type has good research and understanding going on, as the study can not harvest the human samples, it can be said as underdeveloped. Magnetic resonance imaging and ultrasound are used to test the joints and accumulation of the fluid in the synovial joints.
Spondylitis and Sacroiliitis
- The inflammation can arise anywhere from the neck to the lower back to the least vertebra. The whole spinal column to the tailbone is at risk of being affected in this condition. Inflammation spreads from the neck to the spinal column, vertebrae, pelvic areas of the sacroiliac area, discs, and joints on the pelvic floor.
- The tissues, ligaments, and connective tissues associated with the areas also become inflamed. Arms, buttocks, thighs, legs, and feet are affected badly.
- It occurs in 5 percent of the patients with psoriatic arthritis, also men being the main target.
- In this condition, vertebrae are affected asymmetrically unlike the ankylosing spondylitis.
- Paravertebral ossification is seen forming bone structures into the soft tissues around them. Disc calcification results in vertebral fusion and also neurologic complications because of the misalignment of the joints in the spine, and stiffness of the lower backbones. Sacroiliitis pain without stiffness in the lower back can also happen in this type of psoriasis arthritis. Sacroiliitis is an inflammation of the sacroiliac joints of the pelvic.
Enthesitis
- This is an inflammation in the points of articulation which means the points where the ligaments and tendons get inserted into the bone in the joints get inflammation. All the fibrous and fibrocartilaginous, tendons, ligaments, and joint capsules, are inserted into the bones together called entheses.
- An entheses organ consists of fibrocartilage, bursa, fat pad, fascia, and calcaneus bone adjacent to it. The inflammation of the entheses is enthesitis.
- Enthesitis is exclusively found in people with psoriatic arthritis. The most affected regions in our body are the ligaments or sole and foot like Achilles’ tendons, pelvic ligaments, ligaments attached to the ribs, and ligaments of the spine.
- Enthesis results in tissue fibrosis and tissue ossification or calcification. Both in rheumatoid arthritis and osteoarthritis, enthesitis, and dactylitis, cannot be noticed. They are seen only in psoriatic arthritis conditions.
- It is why it is called the hallmark of psoriatic arthritis.
- Instead, Spondylitis can be seen in both cases including psoriatic arthritis commonly.
Psoriatic arthritis mutilans
- It is the most severe yet rarest kind of psoriatic arthritis with one to five percent cases. It can be as severe as rheumatoid arthritis. It is characterised by the pencil-in-cup appearance. The digits appear so with the joints getting dissolved.
- Severe arthritis mutilans show involvement of flexion, third, fourth, and fifth digits. Both the distal interphalangeal predominant psoriatic arthritis and psoriatic arthritis mutilans are typical of dactylitis. Dactylitis as talked about before is the legit mark of psoriatic arthritis apart from the major symptoms like back pain, swollen toes, and feet, etc.
- The opera-glass hand is the common symptom of arthritis mutilans in men over women.
How to Diagnose Psoriatic Arthritis?
For diagnosing a psoriatic arthritis case, one should consult a rheumatologist. They deal with such inflammatory diseases. No blood tests are done to identify the type of psoriatic arthritis. All of the patterns of psoriatic arthritis mentioned above are scaled on scores. Each of them has an established analogue scale to assess the range of symptoms.
- The score of current psoriasis, a history of ps, psoriasis in the family, the inheritance pattern, the patient history of psoriasis, the dactylitis examination, examination for new bone formations, testing negative for rheumatoid factor, and nail dystrophy are essential to list to be assessed for psoriatic arthritis.
- On primary examination, a few x Rays or MRIs are prescribed for diagnosis. The new formations around bone and joints, deformities, etc, can be traced through those investigations. The uric acid quantity is taken into consideration as in gout disease to estimate the extent of inflammation. Ultrasounds can also be prescribed by the rheumatologist if needed. Blood tests are rarely asked for, in the case of monitoring therapies.
- All the radiographic findings look for joint space narrowing, fluffy periostitis, soft tissue swell of, sacroiliitis, enthesitis, erosion, synovitis, inflammation of small joints, pencil in cup deformity, and also intervertebral bony bridges in the spine.
- Lab findings include serum immunoglobulin tests, rheumatoid factor test, erythrocyte sedimentation rate and c reactive protein levels test, and complete blood count.
Psoriatic arthritis if neglected can attract various other problems with it like deformation of fingers and toes, obesity, high blood pressure and high uric acid, inflammations of the eyes, nerves, blood vessels, cardiac diseases, depression, stress, bone density changes, atherosclerosis and skin diseases becoming chronic and unyielding.
Treatments for psoriatic arthritis:
The treatments for psoriatic arthritis are more of a regimen to follow. All of them assure a relaxation from the aggravating disease symptoms. However, they are prescribed based on the patient’s health history, budget, disease activity, severity, patient choice, comorbidities, lifestyle, and mental strength. Whatever the treatment plan is, a consistent regimen is necessary for relief from the symptoms.
- DMARDS are disease-modifying antirheumatic drugs. These classes of drugs are indicated for the treatment of inflammation and inflammatory diseases. Especially utilized in treating rheumatoid arthritis and psoriasis arthritis, they have been proved well for the management. Although there are many options like sulfasalazine, cyclosporine, leflunomide, and other biologic agents belonging to this class, methotrexate is considered the best.
- Methotrexate is the most commonly used DMARD at the beginning of the treatments. This specific class of drugs is utilized in the treatment plan for the remission of the disease, to lower the disease activity and severity, and also to halt the further progression of the disease. The treatment for arthritis can either be combination therapy or monotherapy, but uses disease-modifying anti-rheumatic drugs as an agent.
- Secukinumab is an interleukin. It has been used for treating inflammatory diseases such as psoriatic arthritis, psoriasis, and so on for many years. Inflammation is the common symptom of all these diseases. They have inflammatory cytokines which are like signaling molecules that tell the body to produce more immune cells ending up in inflammation. Thus these are responsible for the pathogenesis of the disease. Secukinumab is a fully monoclonal antibody and selectively targets inflammatory cytokines. They act effectively to the action at the specified tissues. These targeted biological therapies are replacing immunosuppressants vastly with their efficacy. Biologics like interleukin 1,2 and 23, interleukin 17 are taken advantage of.
- The treatment strategy begins with non-steroid anti-inflammatory drugs also called NSAIDs along with local glucocorticoid injections as initial therapy. For the patients with joint damage, such as dactylitis, poly or monoarthritis, or oligoarthritis the treatment demands the rapid use of conventional systemic disease-modifying antirheumatic drugs.
- If the desired immune suppression is not achieved by this, biologics come into plan. The biological disease-modifying antirheumatic drugs that target the specific cytokines are opted for. Interleukin 12/23, interleukin 17A if necessary a tumor necrosis factor inhibitor, TNF also should be used as the first line of treatment. If the biologic DMARDs also fail, the Janus kinase inhibitors are introduced primarily.
- For a person with mild disease, phosphodiesterase -4 inhibition is proposed for patients.
The management of psoriasis arthritis is both non-pharmacological and pharmacological. Keeping the musculoskeletal aspects of the disease, severity, and spread, recommendations of these drugs vary.
Read More About
Reference:
- https://emedicine.medscape.com/article/2196539-overview
- https://www.ncbi.nlm.nih.gov/books/NBK507863/
- https://emedicine.medscape.com/article/2196539-overview
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7286048/
- https://www.sciencedirect.com/science/article/abs/pii/S0190962221024944
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8572231/
- https://www.sciencedirect.com/science/article/pii/S0049017216300646
- https://www.sciencedirect.com/science/article/abs/pii/S0049017221002304
- https://www.sciencedirect.com/science/article/abs/pii/S0190962221003431
- https://www.medicalnewstoday.com/articles/326823
- https://www.sciencedirect.com/topics/medicine-and-dentistry/arthropathy
- https://www.sciencedirect.com/science/article/abs/pii/S0049017221002304
- https://www.sciencedirect.com/science/article/abs/pii/S0190962221003431
- https://emedicine.medscape.com/article/2196539-overview#a3
- https://www.nature.com/articles/nrrheum.2017.188
- https://www.sciencedirect.com/science/article/pii/S0049017217306273
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1846724/
- https://www.sciencedirect.com/science/article/pii/B9780323524834500491
- https://www.sciencedirect.com/science/article/pii/S0049017216300646
- https://www.sciencedirect.com/topics/medicine-and-dentistry/arthropathy
- https://www.sciencedirect.com/science/article/abs/pii/S0190962221003431
- https://emedicine.medscape.com/article/2196539-guidelines
- https://emedicine.medscape.com/article/2196539-treatment
- https://www.medscape.org/viewarticle/565547_4
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7286048/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7360582/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6251836/
- https://www.ncbi.nlm.nih.gov/books/NBK507863/
- https://www.medscape.org/viewarticle/565547